In the past decade, nearly 1.8 million people in the United States lost their lives by suicide or alcohol and drug consumption. Collectively, these deaths are sometimes referred to as “deaths of despair”, a term that emphasizes economic and social deterioration as driving factors. However, additional and more complex factors may be linked to these deaths, such as health disparities, challenges with treatment access, reduced public services, and changes in drug supplies. Therefore, the term “substance use and suicide deaths” is used throughout this brief as a composite measure describing deaths due to alcohol, drugs, and/or suicide. These causes are examined together because they share many upstream risk factors and prevention strategies related to mental health and substance use.
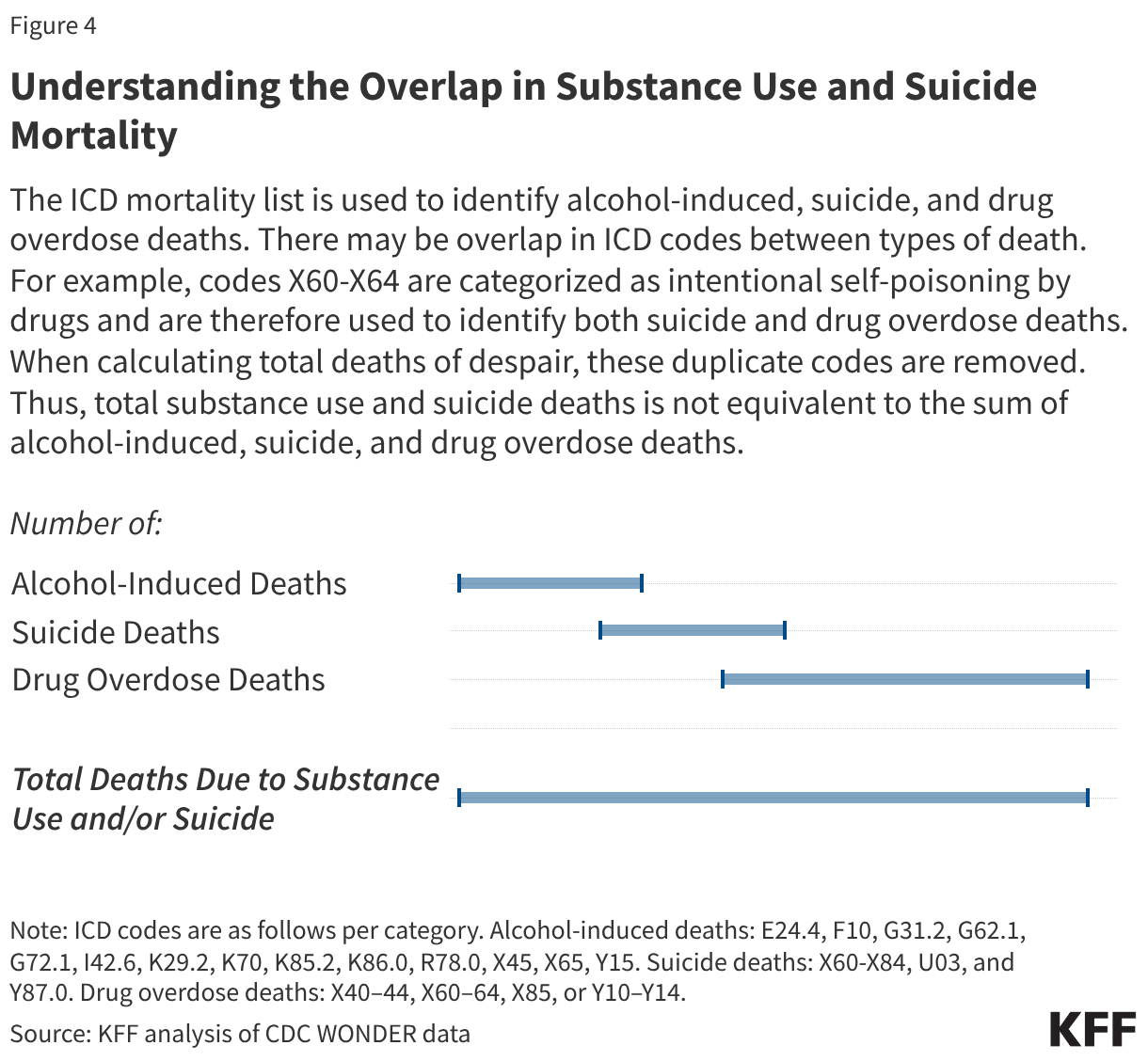
This analysis explores trends in substance use and suicide mortality using data from CDC WONDER. Due to overlap in several ICD-10 codes for deaths involving drugs, alcohol and/or suicide, duplicate codes were removed. Therefore, total substance use and suicide deaths are not equivalent to the sum of alcohol-induced, suicide, and drug overdose deaths (see Methods for more information). Key takeaways include:
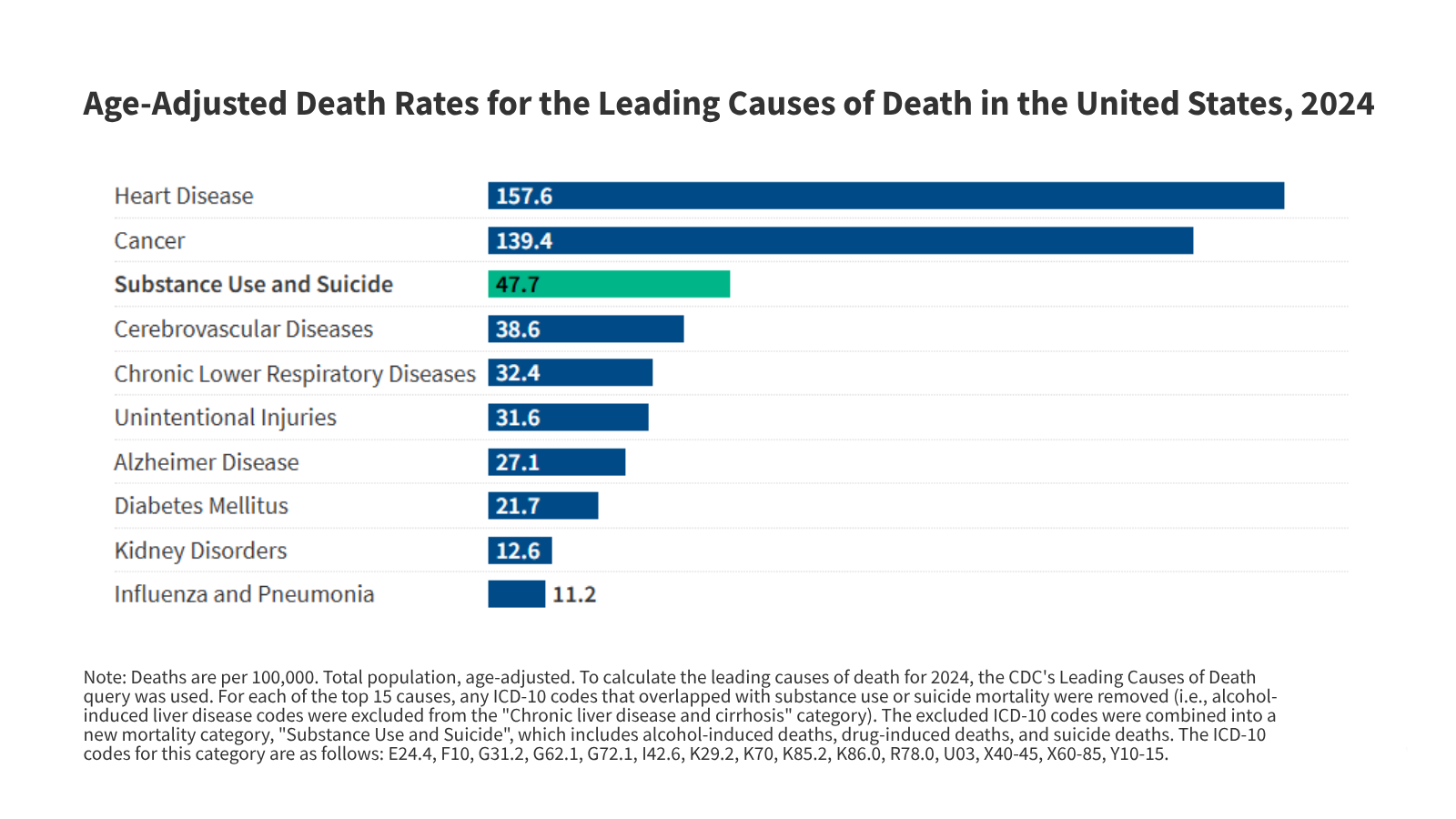
- In 2024, substance use and suicide deaths (47.7 per 100,000 population) were the third leading cause of death in the U.S., behind heart disease (157.6) and cancer (139.4).
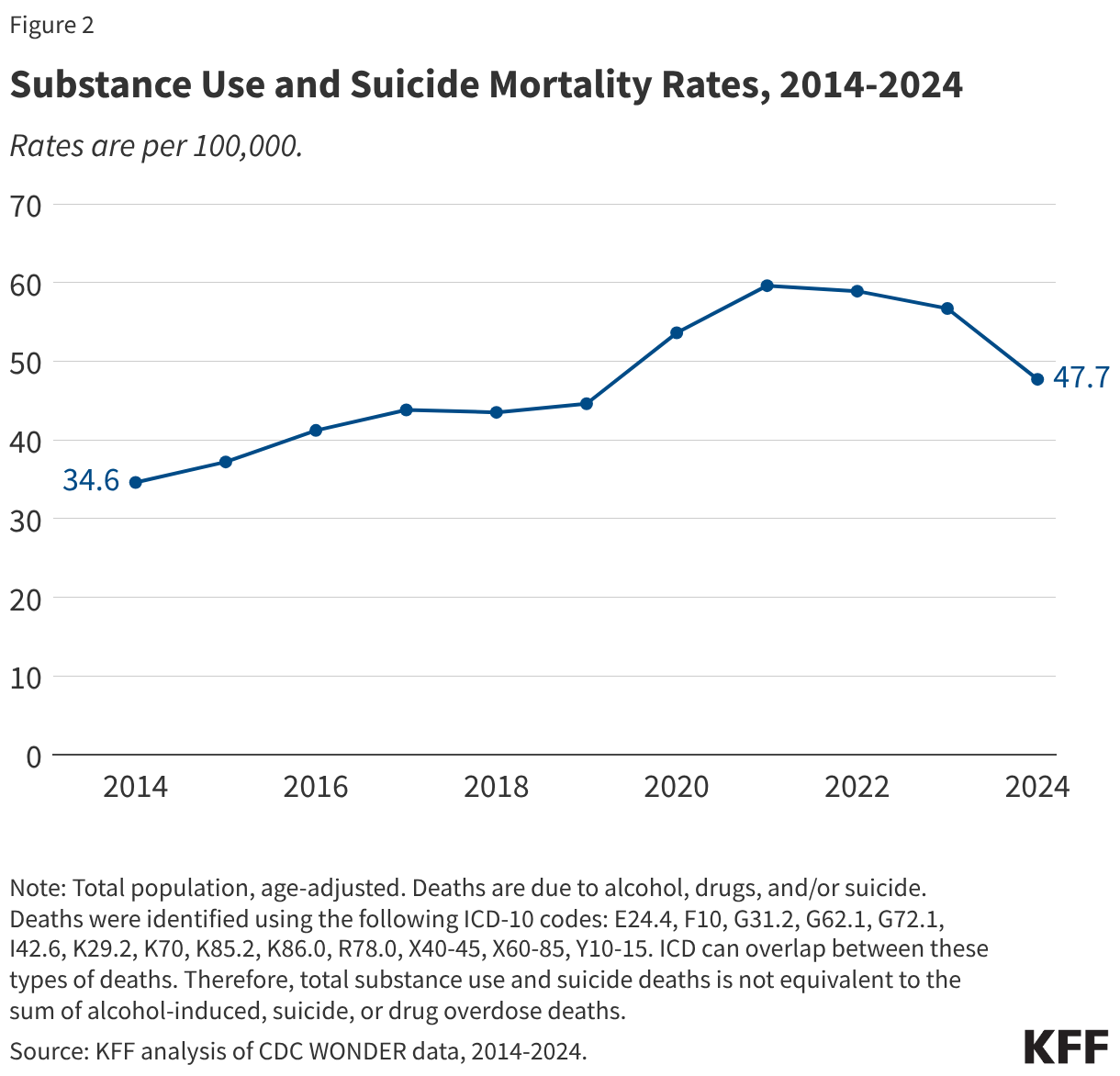
- Deaths due to substance use and suicide increased over the past decade (34.6 in 2014) and peaked during the pandemic (59.6 in 2021).
- Older adults, men, and some communities of color were disproportionately impacted by substance use and suicide deaths compared to their peers.
Despite these high mortality rates, many individuals experience challenges obtaining mental health and substance use services. KFF analyses found that while health insurance is linked to increased utilization of mental health services, many insured individuals do not receive needed mental health treatment. This is associated with multiple factors, including narrow provider networks, coverage limitations, and cost and logistical barriers. A recent KFF survey found that 19% of adults with health insurance rated their insurance negatively based on the availability of mental health providers, and 43% of individuals with poor mental health said they did not receive needed services or medication in the previous year.
The passage and evolution of the Mental Health Parity and Addiction Equity Act (MHPAE) have sought to reduce some access burdens by requiring health insurance plans to provide benefits for mental health and substance use services in alignment with the benefits provided for medical and surgical care. However, enforcement of MHPAE policies is challenging and recent efforts to modify enforcement practices have been slowed under the second Trump administration. Other policy actions under the Trump administration are impacting access to mental health and substance use services. This includes the 2025 reconciliation law which will reduce Medicaid and ACA coverage, narrowing the scope of federal leadership capacity in mental health and substance use services, and a departure from harm reduction services. Collectively, these changes may disrupt access to and continuity of care at a time when substance use and suicide deaths remain elevated.
1. Substance use and suicide deaths combined were the third leading cause of deaths in the United States in 2024.
In 2024, 170,449 people in the U.S. died from suicide and/or substance use. This translates to an age-adjusted death rate of 47.7 per 100,000 population. Compared to other leading causes of death in 2024, only heart disease and cancer rates (157.6 and 139.4, respectively) have higher age-adjusted rates than suicide and substance use (Figure 1).
2. Over the past decade, substance use and suicide mortality rates increased by nearly 40%.
From 2014 to 2024, substance use and suicide death rates increased from 34.6 per 100,000 population to 47.7 (Figure 2). During this period, death rates increased until 2017 and then held steady before sharply increasing alongside the pandemic (59.6 deaths per 100,000 in 2021). It is likely that the worsening opioid crisis, and specifically the presence of fentanyl in the drug supply, significantly contributed to the spike in substance use and suicide mortality rates during the pandemic. These death rates have declined since peaking in 2021 but remain above pre-pandemic levels (47.7 in 2024 vs. 44.6 in 2019).
3. Substance use and suicide mortality rates have disproportionately affected adults ages 45 to 64, men, and certain communities of color.
From 2014 to 2024, substance use and suicide mortality rates were highest among adults ages 45 to 64 (85.3 per 100,000) (Figure 3). These adults along with adults ages 26 to 44 experienced the sharpest increases in mortality rates during the pandemic. Although these rates have since decreased, they remain above pre-pandemic levels for both age groups. In comparison, young adults (ages 18 to 25) and elderly adults (ages 65 and above) experienced smaller increases in substance use and suicide mortality rates during the pandemic. By 2024, the mortality rate among young adults decreased to 27.2, similar to its rates a decade earlier. However, mortality rates among elderly adults have remained relatively steady since their slight increase during the pandemic.
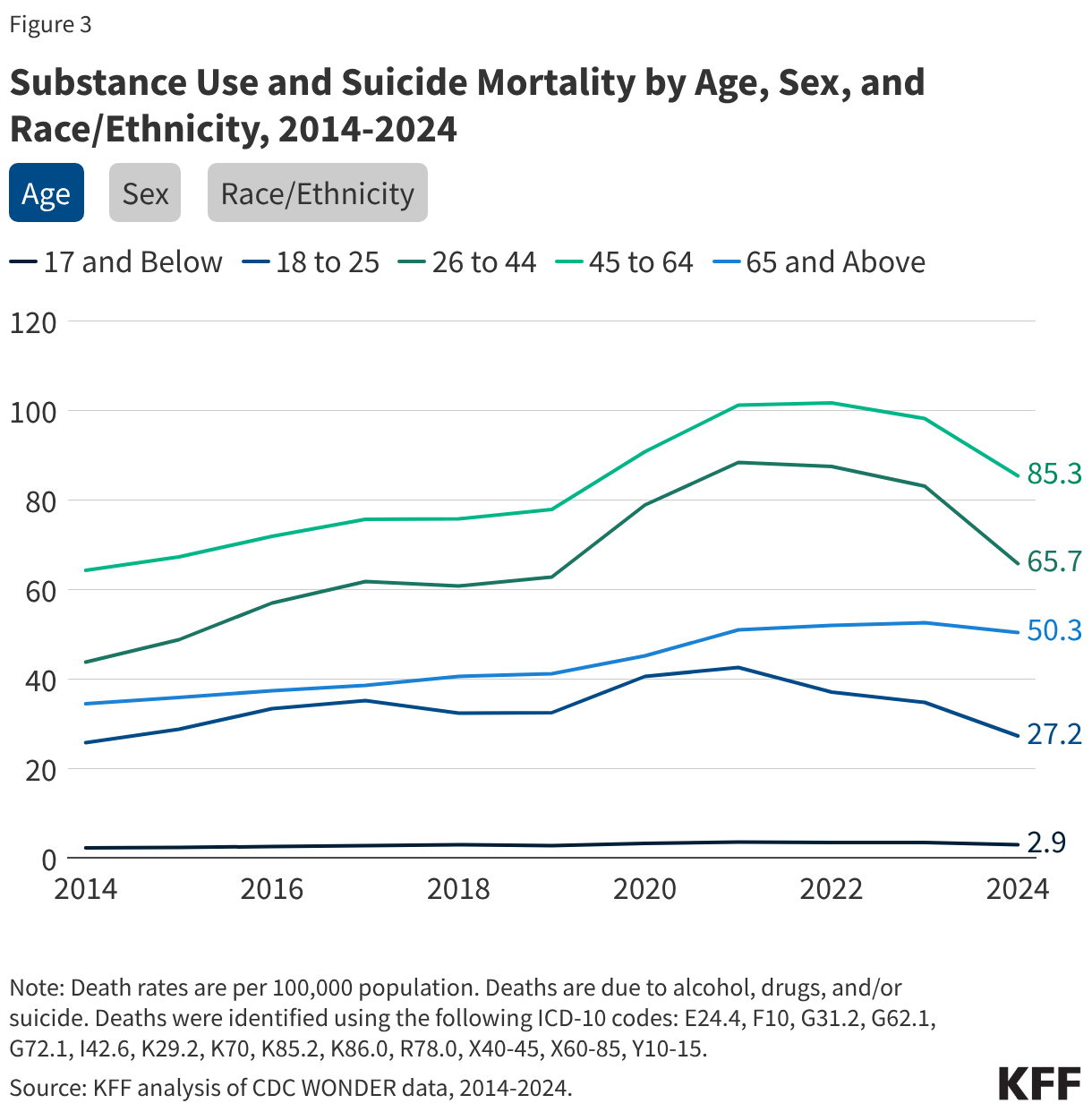
The rate of substance use and suicide mortality among males grew 40% from 2014 to 2024 and remained nearly three times higher than the rates among females (70.6 per 100,000 vs. 25.4 in 2024, respectively, Figure 3). Over the decade, the gap in these death rates has generally widened between males and females: from 50.3 per 100,000 for males and 19.7 for females in 2014 to 70.6 for males and 25.4 for females in 2024. While both groups experienced peak rates during the onset of the pandemic, the increase impacted males more than females (87.6 vs. 32.2 in 2021, respectively).
Over time, people of color have experienced a faster growth in substance use and suicide death rates compared to their White peers. From 2018 to 2024, death rates increased by 43% for Black people, 30% for Hispanic people, 28% for American Indian and Alaska Native (AIAN) people, 14% for Asian and Pacific Islanders, and 2% for White people (Figure 3). As a result, the gap in substance use and suicide mortality rates has largely narrowed between White and Black people and, to a lesser extent, between White and Hispanic people. Additionally, AIAN people consistently experience the highest rates of substance use and suicide mortality compared to all other racial and ethnic groups (130.1 per 100,000 vs. 53.7 among White people in 2024).
Methods